What is vesicoureteral reflux?
Vesicoureteral reflux is the abnormal backflow of urine from the bladder into the ureter and up to the kidney. The majority of the time this is a condition with which a child is born. It is caused by an abnormal entry of the ureter into the bladder. As a result the muscle backing of the bladder does not completely cover the ureter and urine backflows toward the kidney. Reflux is graded on a scale from I-V based on the degree of urine backflow.
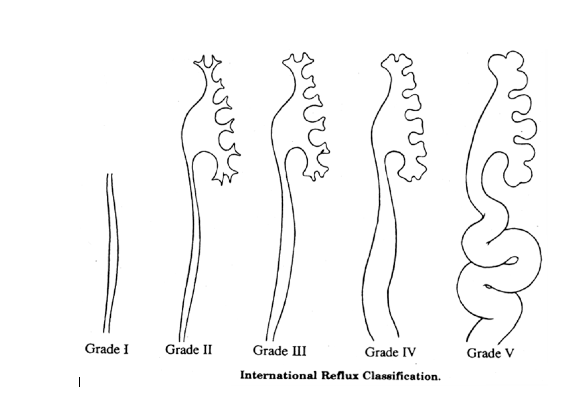
Reflux grading:
Grade I: urine refluxes into the ureter onlyVes
Grade II: urine refluxes into the ureter and up to the kidney without dilation
Grade III: urine refluxes into the ureter and kidney and causes mild dilation
Grade IV: urine refluxes into ureter and kidney and causes dilation without twisting of the ureter
Grade V: urine refluxes into ureter and kidney and causes significant dilation with twisting of the ureter
As the child grows the reflux can decrease or disappear because the entry of the ureter into the bladder further develops and elongates. The lower the grade of reflux the more likely it will resolve on its own. During infancy vesicoureteral reflux is more frequently seen in boys. In the older child vesicoureteral reflux is more often diagnosed in girls.
Vesicoureteral reflux may also occur in children with abnormal bladder function due to nerve or spinal cord problems such as spina bifida. Children with bladder and bowel dysfunction may be more likely to have vesicoureteral reflux. Vesicoureteral reflux can occur in children with other urinary tract abnormalities such as posterior urethral valves, ureterocele, ureteral duplication, or bladder exstrophy.
What are the symptoms of vesicoureteral reflux?
Children with vesicoureteral reflux usually do not have any symptoms or feel sick. Although vesicoureteral reflux is most frequently diagnosed after a urinary tract infection, vesicoureteral reflux does not cause urinary tract infections. Children with vesicoureteral reflux may also have dilation of their urinary tract (hydronephrosis) and sometimes this dilation is detected on prenatal ultrasound leading to radiographic studies after birth that detect vesicoureteral reflux.
How is vesicoureteral reflux diagnosed?
Vesicoureteral reflux is diagnosed by a test called a voiding cystourethrogram (VCUG). This study is performed by placing a catheter through the urethra and into the bladder. The bladder is filled with contrast (x-ray dye) and pictures of the bladder are taken to see if the dye goes backwards up to one or both of the kidneys.
Additional studies that are used in children with vesicoureteral reflux include:
Renal ultrasound: This study is used to determine size and shape of the kidneys.
Radionuclide cystogram (RNC): this test is similar to a VCUG but a different fluid is used to fill the bladder. It is often used as a follow-up study to see if the vesicoureteral reflux has resolved because it is less radiation than a standard VCUG.
DMSA scan: This test provides detailed images of the kidneys to help determine function and condition of the kidneys.
Urodynamics: Occasionally this test is used to determine bladder function, specifically bladder volumes and pressures. Bladder function may contribute to why vesicoureteral reflux is present.
How is vesicoureteral reflux treated?
Vesicoureteral reflux can resolve on its own. Therefore we conservatively manage patients with close follow-up to see if they can outgrow the vesicoureteral reflux on their own. Patients will typically have a cystogram (VCUG or RNC) every 1-2 years to check for vesicoureteral reflux resolution. For patient with higher grades of vesicoureteral reflux or a history of urinary tract infection we often give them a low dose of daily antibiotics (antibiotic prophylaxis) to help prevent urinary tract infection while we are awaiting resolution. Patients who have reflux but have never had a urinary tract infection may be closely followed without antibiotic prophylaxis.
Some children will eventually require surgery for vesicoureteral reflux. The most common reason for surgical intervention is if a child with vesicoureteral reflux has urinary tract infections despite antibiotic prophylaxis.
There are two main surgical interventions for vesicoureteral reflux: ureteral reimplantation surgery (open repair) and endoscopic treatment. (Please see separate handouts)