Introduction
The purpose of this document is to help patient understand that:
- All prostate cancer treatments may have side effects.
- The probability of side effects varies significantly, including their onset (how quickly after the treatment they can occur), severity, and changes over time (how long they might last, whether they might improve, and how quickly).
- Differences in side effects are related not only to the choice or combination of treatments, but also greatly depend on many factors: specific details of the treatment, experience and expertise of the doctor providing the treatment, individual patient factors including age, baseline function, and many other factors. So, it is essential to talk to your treating team about your specific situation to better understand what side effects can be expected in their hands, and their anticipated likelihood and severity.
- Prostate cancer treatments and treatments for side effects are improving over time. Treatments that caused significant side effects in the past might be much less risky today, and even less so in the future.
- Many tools, techniques, and interventions that can help patients overcome or at least manage many side effects.
- Some side effects can have significant impact on a patient’s quality of life. However, even that depends on the individual patient: what one person finds very bothersome may be a minimal concern for another. The goal is to always to maximize your quality of life as you perceive it.
- Side effects impact not only the patient but also their loved ones. It is critical to engage with partners and other close family and friends in the discussions with the team.
Do not suffer in silence! Most side effects of treatment can be addressed, at least partially, using medications, surgical interventions, and/or changes in lifestyle.
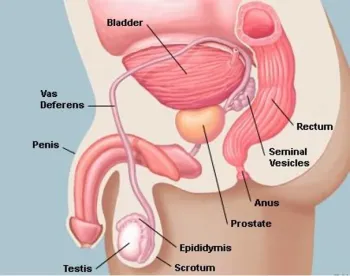
The fundamental challenge in treating prostate cancer is the location of the prostate in the pelvis and the multiple critical structures in its immediate neighborhood. All prostate cancer treatments may, to a lesser or greater extent, damage the urinary sphincter, urethra, bladder, rectum, cavernous nerves, bulb of the penis and other tissues adjacent to the prostate, with risks of effects on urinary, bowel, and/or sexual function. Furthermore, androgen deprivation (hormonal) treatments (ADT) can cause additional side effects. This document covers the most common side effects, techniques to cope with them, and their treatments. Additional information can also be found in the earlier sections covering specific treatments for localized disease.
Each potential side effect has many characteristics that patients should consider and discuss with their treating team and loved ones:
- Probability
- Timing of the onset
- Potential severity depending on patient’s baseline
- How long it might last, and does it typically get worse, better, or stay the same as time progresses
- Is it treatable and what are the treatment options
- Impact on quality of life
Many patients, before getting the treatment, might either underestimate or overestimate the impact of some of the side effects on their quality of life. Discussing it with other patients who have already experienced these side effects can greatly help to improve that understanding, but it’s also critical to bear in mind that every individual’s experience is unique, and that outcomes can vary greatly across different medical centers and clinicians.
Urinary side effects and Incontinence
Urinary tract effects can have a significant impact on a patient’s quality of life. Consequently, early preparation and early treatment of this side effect is extremely important. It’s also important to realize that most men develop at least some decline in urinary function with aging due to benign growth of the prostate (BPH) and/or bladder overactivity. Some men even have incontinence in the absence of any cancer treatment.
There are multiple types of urinary effects:
- Urinary obstruction – difficulty emptying the bladder, takes a long time to empty, etc.
- Stress incontinence – urine leaks occur when one sneezes, coughs, lifts something heavy, or does other things that increase abdominal muscle tone. Stress incontinence can range from a few drops with sneezing to a constant leak.
- Post-void dribbling – Urine leaks at the end of urination, often when a man stands up from sitting or walks away from the toilet/urinal.
- Urgency / frequency / urge incontinence – The bladder loses capacity or is hyperactive and sends signals to the brain to empty when it’s only partially full, requiring a patient to urinate frequently and/or urgently. If the urgency is severe, this can lead to leakage or even complete voiding before reaching the bathroom.
- Overflow incontinence – If the bladder is chronically blocked / overfilled, a patient may experience leakage through frequent dribbling
- Nocturia – specifically voiding frequently at night. This can be due to either obstruction or urinary urgency, and is often multifactorial, with many risk factors including aging.
Depending on the type and level of incontinence there are many different tools and aids, as well as treatments, that can help patients in dealing with incontinence.
It is also important to recognize that the incontinence after radical prostatectomy will resolve in steps. It usually gets better first at night, then when you are up and around. Finally, it improves when you are coughing, laughing, and otherwise increasing your abdominal pressure (stress urinary incontinence - SUI). Many patients might continue to have some limited stress incontinence for a prolonged period of time. Recovery tends to plateau at/around 1 year, so if you are still leaking beyond a year, you should discuss surgical or other interventions. For men with severe leakage (greater than 5 pads per day), early consultation with the reconstructive/cancer survivorship urologist is important to discuss options.
If you have urinary obstruction symptoms, these may often improve after prostatectomy, whereas after radiation therapy they may improve, remain stable, or get worse. In some cases, you should consider a TURP or other procedure to address BPH/obstruction before starting radiation.
Following radiation, there is often a period of increased urinary urgency and/or blood in the urine in the first few months. These symptoms usually resolve, but in some cases persist in the long-term. Symptoms can also develop years down the road, too. Urge incontinence might occur months or even years after the treatment, if at all. Likelihood of long-term urinary side effects can vary quite a bit depending on details of treatment, your treating team’s experience, and your body’s reaction to the radiation (which can be a bit difficult to predict). Incontinence due to radiation treatments, if present, most likely won’t resolve itself without medical intervention.
Managing Incontinence
Kegel (pelvic floor) exercise
In preparation for the treatment that might cause incontinence, patients are advised to do Kegels, or pelvic floor, exercises. These exercises strengthen the sphincter muscle which is responsible for controlling urine flow out of the bladder. After a treatment, once the patient’s doctor gives permission, Kegel exercises are the most important tool that can eventually improve a patient’s continence. Make time for your Kegel exercises; you can do them while standing, sitting, and lying on you back; whenever you do them, focus on a good Kegel for a minimum of 15-seconds each; do ten-reps, take a break and relax, then do some more exercises; keep track of your daily total. Limiting your Kegels right after your catheter is removed is fine (maybe 5 per set); focus on good Kegels, add repetitions as days increase since surgery, and look for improved control and fewer trips to the toilet. Initially, try to practice your Kegel exercises right after using the toilet, when your bladder is empty! Try doing Kegels while visiting the toilet; once you start to urinate, flex your sphincter muscles and stop the flow; repeat this for "extra credit" (you may have found a shortcut to the finish-line). A good physical therapist might help you develop better Kegel technique if you are struggling. Some patients have had good results from doing Kegel exercises while walking. At the same time, it’s important to remember that overdoing Kegel exercising can lead to muscle fatigue and urine leakage.
Men who carry significant weight in the belly can experience higher pressures in the abdomen which can translate to more pressure on the bladder, exacerbating leakage. Weight loss and increased overall fitness can help with urinary symptoms over time, at least to an extent.
There are additional resources that can help you learn how to properly perform Kegel exercises: https://www.ucsfhealth.org/education/pelvic-muscle-exercises
More from Dr. Lindsay Hampson with illustrations here.
And Dr. Hampson suggests men check out www.fixincontinence.com
Skincare products
Incontinence can produce skin irritation so it’s important to maintain good skin hygiene which can include skin products that can prevent or treat skin irritation. Similarly, catheters, pads and diapers, penile clamps, and condom catheters can irritate skin. Products can be classified into two categories: skin sealants or moisture barriers, and antiseptic agents. Skin sealants/moisture barriers include many products, and use is based on potential allergies and personal preferences. They can contain lanolin, zinc oxide, silicone, or petroleum jelly. They are typically applied using sprays or towelettes. Use of antiseptic agents are an important part of care, especially while using a catheter. The most common products are chlorhexidine and iodine.
Pads, diapers, and underwear
While dealing with incontinence, patients can use diapers and pads (similar to women’s menstrual liners) to capture urine while leading a normal life. Most men find pads to be the most convenient way to deal with incontinence. There are many different pad and diaper options and it’s quite easy to find online and in almost any drugstore an option for these products with the right fit and right absorbency level. The options vary from large, bulky diapers that can absorb and capture significant amounts of urine to tiny, thin pads that can handle the entire day of small releases of urine. Patients can also find underwear with built-in washable pads and underwear designed to hold removable pads. As different patients have different preferences, it’s useful to investigate options ahead of time. Experimenting with different methods and types of garments to control leakage can help you find the best personalized approach for you.
Bed, chair, and car seat protection
Drugstores also carry various products that can be used to protect beds, car seats, and chairs from potential urine leaks. These pads can be put under a bed sheet or on a chair to create a waterproof barrier and to absorb potential urine leaks while in bed or sitting in a chair.
Penile clamp
Penile clamps are an effective method to control incontinence. They provide external pressure on the urethra preventing urine leakage. They are particularly effective during exercise or a brief activity where you want zero leakage such as a social gathering. Typically, manufacturers recommend to reposition clamps every 2 – 3 hours (each time when urinating). They are usually very well tolerated and are very effective. Clamps can cause, however rarely, penile inflammation or skin ulcers. They are likely best used for short intervals like an hour or 2, although many men have had success using them throughout the day as long as the location is rotated. There are a few different types, and patients can choose them based on their personal preference. A wide variety are available on Amazon and can be obtained without a prescription.
Condom catheter, also called male external catheter
Condom catheter consists of a few parts: a condom-like tube that is put over the penis, similar to a condom, a urine collection bag that is typically attached to the thigh, and a small tube that allows urine to flow from the condom catheter on the penis to the collection bag. The catheters are available in different sizes and from different materials. Some are attached using a special, skin safe, glue, some are self-adhesive, while some don’t require any glue. They are very effective but can get in the way while participating in some sports. Afex underwear system, available on Amazon, is similar to a condom catheter but in a reusable system that’s washable.
Incontinence Treatments
Surgical Interventions for stress incontinence
Transurethral Balloon
A Transurethral Balloon is a minimally invasive procedure used to treat stress urinary incontinence: two balloons are placed near the bladder neck. The fluid-filled balloons support the bladder neck to prevent urine leakage. A port, used by a doctor to adjust the balloon volume during clinic visits, is placed under the skin of the scrotum.
Bulking
For men with 1 pad per day, urethral bulking with Bulkamid can improve leakage with few side-effects. This can be done in the office or operating room. With a scope and camera through the urethra, a material is injected near the urinary sphincter to allow the sphincter to work better. Some men only experience transient improvement.
Sling
The sling acts as a hammock to lift or support the urethra and sphincter muscles. Slings are made of mesh and can be placed through a perineal approach (between the anus and the scrotum). Years after insertion of the sling, in some rare cases, patients might experience urethra erosion which could require surgical intervention. Most men will experience some decline in control with slings over time. Sling placement is a quick and straightforward outpatient procedure, but is only typically effective for mild to moderate leakage (i.e., for men who require 1 to 2 pads per day).
Artificial Urinary Sphincter
AUS or Artificial Urinary Sphincter places a device with three parts into the body:
- Cuff (a fluid-filled artificial sphincter) that is placed around the urethra,
- Ballon (filled with the same saline as the cuff) that is inserted in the pelvis and used to regulate pressure
- Pump that is placed in the scrotum and used to control urination by inflating and deflating the cuff.
When the pump is squeezed, the fluid in the balloon moves out of the cuff of the artificial sphincter, allowing the urine to flow. The cuff slowly refills with fluid and closes the urethra to stop leaks. When the AUS is placed, the sphincter is de-activated (i.e., does not work and baseline leakage continues) for 6 weeks after surgery to allow the urethra to heal. The AUS, similar to the sling, takes 90 minutes and is an outpatient (come and go) procedure. After 6 weeks the device is then activated, and the patient is shown how to use the device. The AUS is more effective than the sling for men with more significant levels of leakage. Both are associated with low risks of urethral erosion over time. While slings aren’t effective in patients who have had radiation, AUS can work well for radiated patients. Radiation can make the AUS lifespan shorter. Some men will need revisions of the AUS years after implantation due to the system losing fluid and tissue atrophy.
Treatments for urgency/urge incontinence
There are many medications that can be quite helpful in reducing urgency, frequency, and urge incontinence caused by an overactive bladder. Medications for stress incontinence tend to be less effective. These drugs have side effects that vary, depending on what drugs are used. If you would like to consider drug-based control of your incontinence, you should talk to your doctor about the applicability of that treatment and potential side effects.
When medications are not sufficient or cause side effects, other alternatives include injections of Botox into the bladder and neuromodulation through either electroacupuncture at a point above the ankle (“PTNS”) or implantation of a small stimulator device in the back.
Strictures
Urethra stricture is a narrowing of the urethra caused by the development of scar tissue. Strictures can develop after prostate cancer treatment including radical prostatectomy and radiation therapy. They are much less common following robot-assisted as opposed to open prostatectomy. They are uncommon after radiation as well, but can develop years after radiation.
Repetitive damage of the urethra caused by radiation therapy can lead to fibrotic changes in the tissue of the urethra causing narrowing of the urethra.
Symptoms can include a weak urine stream, spraying urine, and finding it hard or painful to pass urine. This, in turn, can lead to urinary urgency, incontinence due to an overactive bladder, or overflow of a full bladder, and bladder infections.
Strictures are diagnosed using X-ray imaging, a urine flow test, ultrasound, MRI, cystoscopy (a small flexible scope with a camera that is inserted into the urethra), or voiding cystourethrogram (examination of urine flow using contrast).
Strictures Treatment
Surgical Intervention
Most mild strictures can be addressed with minor procedures under light anesthesia including dilation or endoscopic incision, i.e., cutting the stricture through the urethra and avoiding any incisions in the skin. Based on the results of diagnostic procedures, if the stricture is more severe, a urethral reconstruction might be necessary. During the procedure, called urethroplasty, scar tissue is removed and then the two healthy ends of the urethra are stitched together. In cases where the gap is too large and the ends cannot be stitched together, a patient’s tissue is used to reconstruct a portion of the urethra. The most common tissue used is taken from the inside cheek of the patient’s mouth.
After the surgery a catheter is placed for three to four weeks, and later, tests are performed to determine if the repair has healed and to measure urine flow rate.
Gastrointestinal side-effects
Radiation proctitis
Inflammation of rectum (radiation proctitis) may occur as a result of radiation therapy. The risk of developing the symptoms depends on technical factors including the dose received by rectum, as well as the individual body’s response to radiation. It can be acute, occurring relatively early after the treatment, or chronic, occurring months or even years after the treatment. Patients experience bowel obstructions, bleeding, and/or stricture formation. Diagnosis requires a digital rectal exam, in extremes performed under anesthesia.
Treatments of acute proctitis include topical use of sodium butyrate, mesalamine, or corticosteroid enemas. Chronic proctitis can also be treated. Treatments include sucralfate enemas, formalin application, glucocorticoid suppositories, as well as hyperbaric oxygen therapy.
Fissures (not common)
The tears can be extremely painful and can cause bleeding with bowel movements and after a bowel movement. Pain can last from several minutes to hours after bowel movements.
The majority of anal fissures don’t require surgical intervention. The most common treatment is making stool softer by increasing intake of fiber through changes in diet or an over-the-counter fiber supplement. Use of stool softeners and increase of water intake also helps.
To relieve pain, topical anesthetics and warm tub baths (sitz baths) are used.
Non-surgical treatments include nitroglycerin ointment and calcium channel blockers. Both increase blood flow to the injury site accelerating healing of the fissures.
In more severe cases surgical options include Botox injections and surgical division of a portion of the anal sphincter. While the procedures are relatively safe, in some rare cases they can lead to fecal incontinence.
Fistula (Not common)
Fistula is a very rare but serious complication treatments of prostate cancer. Fistulas are holes opening between the rectum and urinary tract. They can lead to serious chronic infections, debilitating groin pain, and urinary obstruction.
Fistulas are diagnosed using an MRI and are treated through surgical reconstruction.
Sexual Dysfunction
Treatment side effects can include erectile dysfunction (ED), reduction or absence of ejaculation, penile shortening, and decreased libido or sex drive.
Erectile dysfunction (ED), the inability to achieve and maintain a penile erection adequate for sex, is a common side effect of prostate cancer treatment. ED resulting from prostatectomy occurs quickly and often improves over time if nerve sparing is performed. The onset of ED after radiation therapy can occur more slowly, even over years. In addition, erectile function also tends to decrease over time simply as men age. ADT, often used together with radiation, will suppress erections and libido (sex drive). After prostatectomy, orgasm is preserved but there is no ejaculation, and for this reason no fertility. Sperm banking in advance is possible. Ejaculation tends to decrease in volume after radiation too, but more variably. Subjective quality of orgasm can change as well, after both treatments.
Patients’ chances of experiencing any of the side effects, and in particular ED, vary depending on age at the time of treatment, existing and future health conditions, pre-existing erectile function, procedure details, use of ADT, and many other factors.
It is also important to note that almost all men with ED can achieve erections with one of the many ED treatments and aids, including: PDE5 inhibitor drugs such as Viagra and Cialis, vacuum pumps, urethral medication, penile injections, and implanted erection devices (inflatable penile prosthesis).
Consequently, all patients should talk to their physicians to better understand their particular situation, advantages and disadvantages of various treatments, and potential side effects, including ED.
Physicians use a patient’s pre-treatment data to advise on most likely side effects and their extent as a result of specific treatments. This also applies to a patient’s future erectile function. Patients can help their physician by providing the completed questionnaire prior to the first clinic session.
If ED is an issue after treatment, the patient is recommended to consult with a urologist who specializes in ED caused by prostate cancer treatment. Early intervention is recommended.
Erections require blood flow to the penis, so anything that impairs circulation over time (e.g., smoking, obesity, high blood pressure, diabetes) will exacerbate ED. Healthy diet, increased exercise, smoking cessation, and control of blood pressure and blood sugar can all help—and in any case are good things to do for your heart and overall health.
For more information about Erectile Dysfunction and available treatments read Erectile Dysfunction Management.
Fatigue
Fatigue is a common side effect of radiation therapy and hormonal treatments (ADT).
Fatigue caused by radiation therapy typically occurs during the treatment and resolves after a few weeks after the treatment is over. Some patients report continued but lessening fatigue even for several months after the treatment. Some relief is possible with changes in diet, exercise, and in some most acute cases medication. It has been shown that patients who exercise regularly throughout the course of the radiation have less fatigue than those who don’t.
Fatigue caused by ADT can be quite severe and when treatment lasts for a very long time, can have significant impact on the quality of life. Longer-term ADT also increases the risk of heart disease and can cause osteoporosis (loss of bone density) and muscle loss. To combat fatigue and to protect the body from all of these additional dangers of ADT treatment, regular exercise is extremely important, and should include weight bearing and aerobic exercise regimens.
Other ADT Side Effects
In addition to fatigue, ADT treatment can have many side effects. This includes hot flashes, erectile dysfunction, mood changes, muscle loss, weight gain, anemia, osteoporosis, diabetes, insomnia, cognitive impairment, and heart disease.
Hot flashes management and treatment include many behavioral and medical approaches. It’s important to keep records of triggering factors of hot flashes (alcohol, tobacco, caffeine, spicy food, etc.) and avoid them. Patients can also use environmental cooling (AC, fans, open windows, etc.). Wearing multiple layers to be able to regulate body temperature by removing layers when needed is also an effective approach. In addition to exercising, cognitive-behavioral therapy has also shown good results.
There are also many reports of acupuncture providing significant relief to many patients.
Medical approaches include using intermittent ADT treatment, transition to different ADT drugs or their combination, administering estrogen, progesterone, serotonin reuptake inhibitor, as well as other drugs. Any medical approach should be discussed with a patient’s physician.
Again, be proactive in discussing all side effects with your treating team, no matter when they occur. Many can be solved completely, and most can be at least improved. You are in the driver’s seat in defining how important they are to your quality of life.
This article was written by UCSF patient advocate Leszek Izdebski, with input from UCSF medical expert Matthew Cooperberg, MD, MPH and other members of the UCSF Department of Urology, in December 2024.